Department of Human Services Child Abuse Investigation Letter
•
0 likes•1 view

Here are the key points about your home medications from this visit: - You were prescribed Amoxicillin 400 mg/5mL oral suspension. Take 600 mg by mouth every 12 hours for 10 days. - You were also prescribed Children's Motrin 100 mg/5 mL oral suspension. Take 150 mg by mouth every 6-8 hours. - It is important to take these medications as directed, even if symptoms improve, to fully treat the infection. - Contact your doctor if symptoms do not improve in 2-3 days or if they worsen. Fever over 102°F or other concerning symptoms may require reevaluation. - Give medications with or without food as able. Shake suspension bottles

Recommended
More Related Content
Similar to Department of Human Services Child Abuse Investigation Letter
Similar to Department of Human Services Child Abuse Investigation Letter (20)
More from Roxanne Grinage
More from Roxanne Grinage (20)
Recently uploaded
Recently uploaded (20)
Department of Human Services Child Abuse Investigation Letter
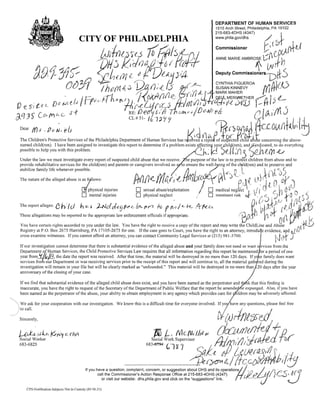
- 1. DEPARTMENT OF HUMAN SERVICES 1515 Arch Street, Philadelphia, PA 19102 215-683-4DHS (4347) I. CITY OF PHILADELPHIA www.phila.gov/dhs '/rD1" I(;d(j~' 61 {;, ,() "j1~ -< chi /J1,[ ~Jf, VfJl1.~("fJ '-4- Deputy commiSSioners'-pfi' S (Ju,.,/1 / h()'(ri.4.3 ~I") . f~ r: /) ~Q~. L/fl,i7r.( v~£,,;- ,f~ :-t1, . -~/~I /if} e: r ,'/,I..,1.A.I ) 1.PA:fI' , u. I': jF. CYNTHIA FIGUEROA SUSAN KINNEVY MARK MAHER 'I .»: /1(' IY1tr i "'- 1" L ",lU D e s. t~ t» el s / r- 1-'-( t'- ~ (,,,e,L-)(y('i'L5 ,-}rn ,(j/ J+(f{-;f;tt·e ,I, QEI/l MERIWETHER L fJ' n::> J'VJ.) I- f} V ~q j!)- C {I1 t-; C- s·f '(;, . RE:f.Je CL # 51- s,'1) Iha{hcd/Dc.fl/Jeis h, '1a Y r L.. l1"l iI)'iJ'tJ 1 . l/'<- JI !, ,I Dear !f)s. p./J, els 'd ~[b9{l~.~UDUllt.tb;l~ The Children's Protective Services of the Philadelphia Department of Human Services has r~~ed a1~lf ~s~~er~ffd a~I'e concerning the above- named child(ren). I have been assigned to investigate this report to determine if a problem exists affectin¥ y?u~. hilll(re.n), an~~n1.icate. d, .to do everything possible to help you with this problem. ' 3 h.: lC J~JI.:n )~n ll}1..e..,., Under the law we must investigate every report of suspected child abuse that we receive, e purpose of the law is to protect children from abuse and to stabilize family hfe whenever possible. ,., ,A, provide rehabilitative services for the child(ren) and parents or c,aregivers involved so a to ensure the well-being of the c~ild(ren) and to preser.ve and )11t i" /' o . lt~"(, The nature of the alleged abuse is;ZS fI lows: rrr t e. 1/ {I-v ItA!) M I); '" ' { "-" YC:a5fl.e','.{~ . cJ-t.. • ;- , e..;'., .., (:'1 (). l} " ',' (),j ),i/ i~'V ;) physical injunes Omental injunes 0 0 sexual abuse/exploitation physical neglect :' 0 0 medical negle~t " Imminent risk r.;.(f fl d t.~ I () 11""~ r_ ) , I, /" C_ ,J ill ,,1/'1) ,; fi flr 1/..) L tAI'1 'It,,-J tAI,~~I(tJ1:.JiCt) j :~/ The report alleges: t h.:t cJ h O,~' l-Nd d~'fJPd<-b:.. (1/r'l Iv f (Vii Co t-: .4-'fe-D, ",'" (1 1~,,, allegations may be reported to tho appropnat law enforcement officials if appropnate. ( ~ I yl. iff (l pi"', k ''I4'1t~..J J You have certain rights accorded to you under the law. You have the right to receive a copy of the report and may wnte the Childl.ine and Ab9se Registry at POBox 2675 Harnsburg, PA 17105-2675 for one. If the case goes to Court, you have the nght to an attorney, introdu~e evidence, apd 'A,l. i, cross examine witnesses. If you cannot afford an attorney, you can contact Community Legal Services at (215) 981-3700. ~I')~' J I t ~ If our investigation cannot determine that there IS substantial evidence of the alleged abuse and your family does not need or want s rvices from the Department 0 Human Services, the Child Protective Services Law requires that all information regarding this report be maintained or a period of one year from i(; I~,the date the report was received. After that time, the material will be destroyed in no more than 120 days. If y r family does want services from our Department or was receivmg services prior to the receipt of this report and Will continue to, all the matenal gathered during the investigation will remain in your file but will be clearly marked as "unfounded." This material will be destroyed in no more than 20 days after the year anniversary of the closing of your case. Ifwe find that substantial evidence of the alleged child abuse does exist, and you have been named as the perpetrator and t . k that this finding is inaccurate, you have the right to request of the Secretary of the Department of Public Welfare that the report be amende or expunged. Also, if you have been named as the perpetrator of the abuse, your ability to obtain employment in any agency which provides care for ildren may be adversely affected. " We ask for your cooperation with our investigation. We know this is a difficult time for everyone involved. ave any questions, please feel free )w~. . ~/ -" Sincerely, Ir tJ)rI(}ffPti/, J-,()"t.t/1J i; Ke /'fit c·-r.M fj L., {Vlc(1lfIJ,t" dcOAiJJ~#d+:l! Social Worker 683-6825 683-'6'm< G llf i SOCIalWork Supervisor '. i /1~ 1./1 . r7(l1 {.t I ( /1 ",~;,J(t1tb. e,' 11/)".' toe JI, , < '"' <;a.l{ /! " ttveffd!<ti'! /. " _' . /1Je(~ eLl (fcCr)iltlM/p,/!;J If you have a question, complaint, concern, or suggestion about DHS and its operati01-ts~ •...; call the Commissioner's Action Response Office at 215-683-4DHS (4347) or visit our website: dhs.phila.gov and click on the "suggestions" link. .' . I·~~· {? ) 'k' Lil' 'U· I/J }/.0 <:-3. c ', C.....:..)' IJ CPS-Notification-Subjecls ot in Custody (8S·M·21)
- 2. Deaysia Daniels-Thomas MRN: 25422718 Temple University Hospital 3401 N. Broad Street Philadelphia, PA 19140 (215) 707-3467 Discharge Instructions for: Daniels-Thomas, Deaysia Arrival Date: Wednesday, March 24, 2010 Thank you for choosing Temple University Hospital for your care today. The examination and treatment you have received in the Emergency Department today have been rendered on an emergency basis only and are not intended to be a substitute for an effort to provide complete medical care. You should contact your follow-up physician as it is important that you let him or her check you and report any new or remaining problems since it is impossible to recognize and treat all elements of an injury or illness in a single emergency care center visit. Care provided by: CALVO, CARMELA, MD Diagnosis: Middle Ear Infection; Viral Illness DISCHARGE INSTRUCTIONS FORMS Ear - Middle, Infection (Otitis Media), Child Medication Reconciliation Viral Illness FOLLOW UP INSTRUCTIONS PRESCRIPTIONS Private Physician Amoxicillin When: 1 - 2 days; Reason: If symptoms persist, Children's Motrin Fever> 102F, Trouble breathing, Recheck today's complaints SPECIAL NOTES None X-RAYS and LAB TESTS: If you had x-rays today they were read by the emergency physician. Your x-rays will also be read by a radiologist within 24 hours. If you had a culture done it will take 24 to 72 hours to get the results. If there is a change in the x-ray diagnosis or a positive culture, we will contact you. Please verify your current phone number prior to discharge at the check out desk; MEDICATIONS: If you received a prescription for medication(s) today, it is important that when you fill this you let the pharmacist know all the other medications that you are on and any allergies you might have. It is also important that you notify your follow-up physician of all your medications including the prescriptions you may receive today. Patient Copy
- 3. Deaysia Daniels-Thomas MRN: 25422718 FOLLOW UP INSTRUCTIONS Private Physician When: 1 - 2 days Reason: If symptoms persist, Fever> 102F, Trouble breathing, Recheck today's complaints PRESCRIPTIONS Amoxicillin 400 mg/5mL Oral Suspension for Reconstitution Take 600 mg by ORAL route every 12 hours for 10 days Children's Motrin 100 mg/5 mL Oral Suspension Take 150 mg by ORAL route every 6-8 hours
- 4. Deaysia Daniels-Thomas MRN:25422718 Middle Ear Infection, Child (Otitis Media, Child) A middle ear infection affects the space behind -the eardrum. This Middle Ear condition is known as "otitis media" and it often occurs as a complication ofthe common cold. It is the second most common disease of childhood behind respiratory illnesses. AN INFECTION WAS FOUND TODAY IN YOUR CHILD'S: o RightEar o Left Ear HOME CARE INSTRUCTIONS ;.- Continue giving medicine, if prescribed, for 10 days or as prescribed even though your child may feel better after the first few days. ~ Only take over-the-counter or prescription medicines for pain, Eustachian Tube discomfort, or fever as directed by your caregiver. FOLLOW UP with your caregiver as directed. SEEK IMMEDIATE MEDICAL CARE IF: ? Your child's problems (symptoms) do not improve within 2 to 3 days. ~ An oral temperature above 102° F (38.9° C) or a rectal temperature above 103° F (39.4° C); or if the oral temperature remains above 101° F (38.3° C) or the rectal temperature remains above 102° F (38.3° C) for three days. );> You notice unusual fussiness, drowsiness or confusion. ? Your child has a headache, neck pain or a stiff neck. ? Your child has excessive diarrhea or vomiting. ;.- Your child has seizures (convulsions). ;.- There is an inability to control pain using the medication as directed. AGREEMENT BETWEEN PATIENT AND HEALTHCARE TEAM: Your signature on this document represents an understanding between you and the healthcare team that took. care of you today. That means that you: I ;.- Understand these discharge instructions. ;.- Will monitor your child's condition. ;.- Will seek immediate medical care as instructed. Document Released: 09/27/2006 Document Re-Released: 06/05/2009 ExitCare® Patient Information ©2009 ExitCare, LLC. Viral Illness Your exam indicates you have a viral illness. SYMPTOMS ;.- Fever. ;.- Stomach upsets. ;.- Muscle aches. ;.- Sore throat. Page I of9
- 5. Deaysia Daniels-Thomas MRN: 25422718 >- Headache. > Dry cough. » Fatigue. a Antibiotic drugs are not effective in viral illnesses. They are only given when there is secondary bacterial infection. TREATMENT > Bed rest. > Increasing oral fluid intake of clear, non-caffeinated drinks like ginger ale, fruit juices, water, or sports (electrolyte) drinks, and > Medicine to relieve specific symptoms such as cough, pain, or diarrhea. Only take over-the-counter or prescription medicines for pain, discomfort, or fever as directed by your caregiver. . Please call your caregiver if you are not better after 2-3 days of symptom treatment. CALL OR RETURN HERE RIGHT AWAY IF YOUR ILLNESS GETS MORE SEVERE, OR YOU DEVELOP ANY OTHER NEW SYMPTOMS, SUCH AS » A fever above 1030 F (39.40 C). » Vomiting for more than a day. > Severe headache or other pain. > Stiff neck. >- Trouble breathing. >- Visual problems. >- "Blackouts" or fainting. Document Released: 01/25/2006 Document Re-Released: 06/05/2009 ExitCare® Patient Information ©2009 ExitCare, LLC. IMPORTANT NOTE: This is a summary and does not contain all possible information about this product. For complete information about this product or your specific health needs, ask your health care professional. Always seek the advice of your health care professional if you have any questions about this product or your medical condition. This information is not intended as individual medical advice and does not substitute for the knowledge and judgment of your health care professional. This information does not contain any assurances that this product is safe, effective, or appropriate. for you. AMOXICILLIN SUSPENSION - ORAL (a-MOX-i-SIL-in) COMMON BRAND NAME(S): Amoxil, Trimox, Wymox USES: Amoxicillin is a penicillin-type antibiotic used to treat a wide variety of bacterial infections. It works by stopping the growth of bacteria. This antibiotic treats only bacterial infections. It will not work for viral infections (e.g.,.common cold; flu). Unnecessary use or overuse of any antibiotic can lead to its decreased effectiveness. HOW TO USE: Shake the bottle well before each dose. Take this medication by mouth with or without food, usually every 8 or 12 hours, or as directed by the doctor. . Page 2 of9
- 6. Deaysia Daniels- Thomas MRN: 25422718 Discharge Information Home Medication Form Temple University Hospital Temple University Hospital Emergency Department Name: Deaysia Daniels-Thomas Visit Date: 03/24/1022:30 Age: 3 years Gender: Female MRN: 25422718 V~nID:405005630026 Physician: CALVO, CARMELA Thank you for visiting Temple University Hospital. This form contains information about your medications. It is important that you read and understand this information. H ome Md s recor d e d d urmg thl IS e " islt VIS I Drug, Route & Dose Frequency Reason Continue Ibuprofen Oral Yes No PCP Acetaminophen Oral Yes No PCP Route Rate Duration Given At Oral 03/2501:36 p rescnpuons you receive d d urmq your "f " VISIlt : " Drug & Dose Route Frequency Reason Next Dose Amoxiciliin 600 mg Oral every 12 hours Infectious Process Children's Motrin 150 mg Oral every 6-8 hours Home Medications ou should continue to take: Drug, Route & Dose Frequency Reason Home Medications ou should STOP takin Drug, Route & Dose Frequency Reason You should follow up with your primary care physician after discharge regarding continuation of these medications: I Drug, Route & Dose Frequency Reason Notes You will need to see your MD to get refills. PLEASE GIVE THIS FORM TO YOUR NEXT PROVIDER OF MEDICAL SERVICE (DOCTOR, CLINIC, HOME CARE, ETC.) Page 1 of I
- 7. Deaysia Daniels-Thomas MRN: 25422718 your usual dosing schedule. Do not double the dose to catch up. STORAGE: Store at room temperature according to product directions away from light and moisture. Do not store in the bathroom. Keep all medicines away from children and pets. Do not flush medications down the toilet or pour them into a drain unless instructed to do so. Properly discard this product when it is expired or no longer needed. Consult your pharmacist or local waste disposal company for more details about how to safely discard your product. . Information last revised July 2009 Copyright( c) 2009 First DataBank, Inc. Page 9 of9